
Refeeding Syndrome in Incarcerated Individuals With Opioid Use Disorder: A Case Study
Abstract
Refeeding syndrome is a serious metabolic complication that can occur when nutrition is reintroduced after periods of malnutrition, yet it remains underrecognized outside traditional clinical settings. Individuals with opioid use disorder (OUD) may be particularly susceptible due to chronic nutritional deficiencies, irregular eating patterns, and recent caloric deprivation—risks that may be intensified during incarceration. This case describes a 30-year-old incarcerated male with OUD who presented to the emergency department with seizures, severe metabolic acidosis, cardiac arrhythmia, and profound electrolyte abnormalities shortly after intake.
The case highlights the diagnostic challenges of recognizing refeeding syndrome in justice-involved populations, where symptoms can overlap with withdrawal, sepsis, or other acute medical conditions. It further illustrates how even brief periods of nutritional restriction followed by unregulated feeding in custody settings can precipitate life-threatening metabolic consequences. Beyond its clinical implications, this case underscores the intersection of correctional health and public health and the role of both healthcare and custody professionals in identifying risk and supporting safe nutritional practices.
Introduction
Malnutrition is often overlooked in patients with opioid use disorder (OUD), despite evidence suggesting widespread micronutrient deficiencies, including vitamins D, B-complex, C, and minerals like iron, selenium, and zinc (Waddington et al., 2023; Jeynes & Gibson, 2017; García-Estrada et al., 2025). Refeeding syndrome is a potentially fatal metabolic complication that results from the rapid reintroduction of nutrition in malnourished individuals (Persaud-Sharma, 2024). It is traditionally associated with anorexia nervosa, chronic illness, or in populations that are predisposed to situations that may cause malnutrition (De Silva & Nightingale, 2019).
Refeeding syndrome often goes unrecognized in patients with substance use disorders, as the presentation is frequently obscured by withdrawal symptoms or other complications of opioid dependence (Ponzo et al., 2021). These risks may be amplified during acute incarceration, where brief periods of caloric deprivation followed by refeeding can precipitate severe metabolic consequences. This case study describes the clinical presentation and diagnostic challenges of refeeding syndrome in a patient with opioid use disorder during acute incarceration.
Case Presentation
We report a 30-year-old incarcerated male with a history of asthma, PTSD, and fentanyl addiction who was transported from jail. He reported to court well-appearing and was incarcerated roughly 15 hours prior. He suffered two seizure episodes prior to arrival to the emergency department (ED). On presentation to the ED, the patient was noted to be in critical condition demonstrating Kussmaul breathing with a respiratory rate in the 30s and an oxygen saturation of 88—92% and a heart rate in the 130s.
He appeared malnourished with a body mass index (BMI) of 16.2 and he was encephalopathic with a Glasgow Coma Scale (GCS) of 7. He was unable to safely cooperate with his care, so to facilitate further management, he was intubated. Within minutes his tachycardia increased to low 200, and he was found to be in supraventricular
tachycardia (SVT). He was given three doses of adenosine, which led to only momentary improvement. 5 mg Lopressor IV and 50 mEq sodium bicarbonate were given and he returned to a perfusing sinus rhythm in the 130s.
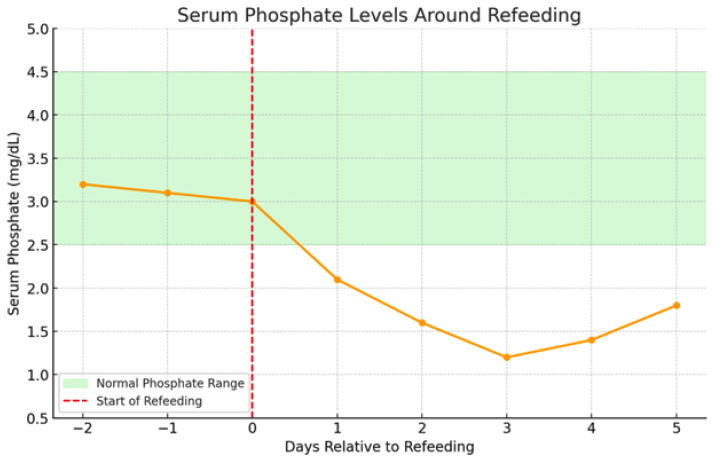
Labs revealed numerous and progressively worsening abnormalities including metabolic acidosis with a pH of 7.00, an anion gap of 37, serum glucose of 262, serum lactate of 22.6, and a serum bicarbonate of 8, raising concern for late onset diabetes mellitus with diabetic ketoacidosis (DKA). Notably, within an hour of admission he demonstrated hypophosphatemia, which progressed to < 1mg/dL. Over time his electrolytes, kidney function, and glucose normalized. Ultimately, his HbA1c was normal. He suffered a type II non–ST-elevation myocardial infarction (NSTEMI) with a nonischemic cardiomyopathy with ejection fraction of 25—30% and an acute kidney injury.
Case Assessment
Our patient with suspected fentanyl withdrawal presented with symptoms mimicking not only diabetic ketoacidosis, but also profound hypophosphatemia, hypokalemia, and hypocalcemia. Given the patient’s acute incarceration and apparent malnutrition, under the pretext that he was fed a high-carbohydrate meal while in jail resulting in critical hypophosphatemia, led us to the consideration of refeeding syndrome as a primary diagnosis. This aligns with the classic presentation of the syndrome
Physiologically, refeeding syndrome hinges on adenosine triphosphate (ATP) depletion from phosphate deficiency. The drop in intracellular phosphate impairs production of 2,3-Bisphosphoglycerate (2,3-BPG), shifting the hemoglobin dissociation curve and worsening tissue hypoxia. The heart, brain, and diaphragm are especially sensitive to these changes. Cardiac irritability from low intracellular potassium and phosphate likely contributed to the patient’s SVT and type II NSTEMI, while lactic acidosis and altered respiratory drive aligned with reduced tissue oxygenation and mitochondrial dysfunction. The cluster of findings coupled with the fact the patient was cachexic and most likely had not eaten in a while, with the reintroduction of the simple carbohydrates during incarceration, strongly supports a diagnosis of refeeding syndrome.
Discussion
Refeeding syndrome is a potentially fatal metabolic imbalance. During starvation, the body switches to catabolizing fats and proteins. With the reintroduction of carbohydrates, the sudden surge of insulin drives phosphate, potassium, and magnesium into cells leading to widespread metabolic and cellular dysfunction (De Silva & Nightingale, 2019). This cascade underpins the classic metabolic crisis seen in refeeding syndrome
(Persaud-Sharma, 2024; De Silva & Nightingale, 2019; Ponzo et al., 2021). Changes like this can cause cardiac arrhythmias, respiratory failure, seizures, and in more severe cases, death. These changes often manifest within 1—5 days after feeding begins and can result in life-threatening cardiac, neurologic, and respiratory complications if not recognized early (Ponzo et al., 2021; Ha et al., 2024).
While refeeding syndrome is well documented in populations such as those with anorexia nervosa or cancer cachexia, it remains underrecognized in patients with OUD. Studies show that OUD is associated with both macronutrient and micronutrient deficiencies, particularly in patients on opioid agonist therapy (Waddington et al., 2023; Jeynes & Gibson, 2017; Furulund et al., 2024).
Opioids alter gastrointestinal function and appetite regulation, promote nutrient-poor food preferences, and reduce food intake overall (Mysels & Sullivan, 2010; Mahboub et al., 2021). Nearly 70% of individuals with OUD have documented vitamin D deficiency, and over half are deficient in folate, Vitamin C, or iron (García-Estrada et al., 2025). These nutritional vulnerabilities, especially during periods of withdrawal or incarceration, may create a high-risk environment for metabolic complications, leading to refeeding syndrome (Wiss, 2019; Ross et al., 2012).
Research shows that individuals with OUD, including those on methadone or buprenorphine therapy, often consume nutrient-poor, carbohydrate-rich diets and experience deficiencies in vitamins A, C, D, E, thiamine, folate, iron, selenium, and protein (Waddington et al., 2023; Jeynes & Gibson, 2017; Furulund et al., 2024). These deficits may be exacerbated during incarceration, where access to nutrition can vary, and abrupt feeding after restriction can trigger refeeding physiology (Mysels & Sullivan, 2010).
Although guidelines exist for recognizing high-risk individuals, they are often under-applied to patients with opioid use disorders due to the myriad of other symptoms or issues they may have, shrouding the true underlying problem. One study noted that up to 74% of patients with opioid use disorder demonstrated significant nutritional deficiencies (Nazrul Islam et al., 2002). Newly incarcerated individuals may experience brief but intense nutritional restrictions, then receive unregulated refeeding in custody or transport settings, making an ideal circumstance for refeeding physiology to manifest silently.
This case is a cautionary reminder that not all anion gap metabolic acidosis in malnourished patients is DKA. In this patient, a normal HbA1C and glucose normalization argued against diabetes. However, severe electrolyte derangements and acid-base shifts misled initial impressions, delaying the correct diagnosis. This case offers a clear illustration of classic refeeding syndrome physiology in a nontraditional, high-risk patient population. The main limitation lies in the lack of a clearly documented caloric intake timeline during detention; however, the rapid and dramatic biochemical response is highly consistent with early refeeding dynamics.
Conclusion
This case highlights the critical need for heightened clinical suspicion of refeeding syndrome in individuals with OUD, particularly those who are incarcerated or have experienced recent periods of caloric restriction. Clinicians must recognize that refeeding syndrome is not exclusive to traditional high-risk groups, such as patients with anorexia or cancer, but may also present subtly in patients with substance use disorders, often misattributed to more familiar conditions such as DKA or sepsis. Early identification, electrolyte monitoring, and cautious nutritional reintroduction are essential to prevent potentially fatal outcomes. This case serves as a reminder that in incarcerated populations, and especially in vulnerable populations where this possibility is often overlooked, silent malnutrition and unregulated feeding can produce life-threatening consequences that demand greater clinical awareness.
Share your voice in our upcoming white paper series on Correctional Health Care as Public Health Care.
Acknowledgements
Evelyn Azbell, CCHP, provided writing assistance, technical editing, language editing, and proofreading.
Author’s Note
All materials have been prepared for general information purposes only. The information presented should be treated as guidelines, not rules. It is not intended to establish a standard of medical care and is not a substitute for common sense. The information presented is not legal advice, is not to be acted on as such, may not be current, and is subject to change without notice. Each situation should be addressed on a case-by-case basis.
Author Disclosure Statement
There are no actual or potential conflicts of interest that may affect the author’s relationships and activities, directly or indirectly, related to the work.
Funding Information
This research received no grant or funding from any agency in the public, commercial, or not-for-profit sectors.
Citation
Gabrilovich, D., Khan, J., & Gabrilovich, M. (2026). Refeeding syndrome in incarcerated individuals with opioid use disorder: A case study. Spark Training. https://doi.org/10.5281/zenodo.18743803
References
De Silva, A., & Nightingale, J. M. D. (2019). Refeeding syndrome: Physiological background and practical management. Frontline Gastroenterology, 11(5), 404–409. https://doi.org/10.1136/flgastro-2018-101065
Furulund, E., Druckrey-Fiskaaen, K. T., Carlsen, S. L., Madebo, T., Fadnes, L. T., & Lid, T. G. (2024). Healthy eating among people on opioid agonist therapy: A qualitative study of patients' experiences and perspectives. BMC Nutrition, 10(1), 70. https://doi.org/10.1186/s40795-024-00880-8
García-Estrada, J., Luquin, S., Pesqueda-Cendejas, K., Ruiz-Ballesteros, A. I., Campos-López, B., Meza-Meza, M. R., Parra-Rojas, I., González-Castañeda, R. E., Ramos-Lopez, O., & De la Cruz-Mosso, U. (2025). Malnutrition in substance use disorders: A critical issue in their treatment and recovery. Healthcare (Basel), 13(8), 868. https://doi.org/10.3390/healthcare13080868
Ha, S. W., Jang, S. H., & Lee, M. J. (2024). Recent advances in refeeding syndrome in critically ill patients: A narrative review. Annals of Clinical Nutrition and Metabolism, 16(1), 3–9. https://doi.org/10.15747/ACNM.2024.16.1.3
Jeynes, K. D., & Gibson, E. L. (2017). The importance of nutrition in aiding recovery from substance use disorders: A review. Drug and Alcohol Dependence, 179, 229–239. https://doi.org/10.1016/j.drugalcdep.2017.07.006
Mahboub, N., Rizk, R., Karavetian, M., & de Vries, N. (2021). Nutritional status and eating habits of people who use drugs and/or are undergoing treatment for recovery: A narrative review. Nutrition Reviews, 79(6), 627–635. https://doi.org/10.1093/nutrit/nuaa095
Mehanna, H. M., Moledina, J., & Travis, J. (2008). Refeeding syndrome: what it is, and how to prevent and treat it. BMJ (Clinical Research Ed.), 336(7659), 1495–1498. https://doi.org/10.1136/bmj.a301
Mysels, D. J., & Sullivan, M. A. (2010). The relationship between opioid and sugar intake: Review of evidence and clinical applications. Journal of Opioid Management, 6(6), 445–452. https://doi.org/10.5055/jom.2010.0043
Nazrul Islam, S. K., Jahangir Hossain, K., Ahmed, A., & Ahsan, M. (2002). Nutritional status of drug addicts undergoing detoxification: Prevalence of malnutrition and influence of illicit drugs and lifestyle. British Journal of Nutrition, 88(5), 507–513. https://doi.org/10.1079/BJN2002702
Persaud-Sharma, D. (2024). Refeeding syndrome. In StatPearls [Internet]. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK564513/
Ponzo, V., Pellegrini, M., Cioffi, I., Scaglione, L., & Bo, S. (2021). The Refeeding Syndrome: A neglected but potentially serious condition for inpatients. A narrative review. Internal and Emergency Medicine, 16(1), 49–60. https://doi.org/10.1007/s11739-020-02525-7
Ross, L. J., Wilson, M., Banks, M., Rezannah, F., & Daglish, M. (2012). Prevalence of malnutrition and nutritional risk factors in patients undergoing alcohol and drug treatment. Nutrition, 28(7–8), 738–743. https://doi.org/10.1016/j.nut.2011.11.003
Singh, J. A., Murphy, S., & Bhandari, M. (2010). Trial sample size, but not trial quality, is associated with positive study outcome. Journal of Clinical Epidemiology, 63(2), 154–162. https://doi.org/10.1016/j.jclinepi.2009.05.007
Waddington, F., Naunton, M., Thomas, J., Kyle, G., Wheatley, B., & Oguoma, V. (2023). Examination of the nutritional intake of patients undergoing opioid replacement therapy: A systematic review. Nutrition & Dietetics, 80(1), 55–64. https://doi.org/10.1111/1747-0080.12784
Wiss, D. A. (2019). The role of nutrition in addiction recovery: What we know and what we don't. In I. Danovitch & L. J. Mooney (Eds.), The Assessment and Treatment of Addiction (pp. 21–42). Elsevier. https://doi.org/10.1016/B978-0-323-54856-4.00002-X